Understanding and Meeting the Unique Needs of Adolescents and Young Adults with Cancer
Over the last 2 decades, there has been an increasing awareness in the United States of adolescents and young adults (AYAs) with cancer being a distinct population with unique needs and challenges. AYAs face poorer cancer outcomes and experiences compared with younger and older cancer patients, and they historically have been lost between pediatric and adult models of oncology care. Formally identified by the National Cancer Institute (NCI) as those aged 15 to 39 years who have been diagnosed with cancer, the AYA population includes approximately 90000 young persons diagnosed annually in the US and 5% of the total annual cancer incidence in this country; it also involves more than 2.1 million current survivors,1 many of whom face decades of late- and long-term treatment effects across biological, psychological, and social domains.2,3 AYAs with cancer have an average 5-year relative survival rate that exceeds 85%, yet they face unique cancer care needs including those related to disparities in health care access, clinical trial enrollment, treatment outcomes, and post-treatment quality of life (QOL) when compared with cancer patients who are not AYAs.4 Mobilized by a desire to improve outcomes and make developmentally appropriate cancer care accessible to all AYAs, many health care providers, patient coalitions, families, foundations, community advocates, and health systems across the country have stepped forward to advocate for care that recognizes and addresses the unique needs of AYAs with cancer.
Improved awareness of the need for AYA-specific care and advocacy has resulted in the development of a subspecialty aimed at improving cancer outcomes and experiences for this patient population. This movement has led to the creation of various hospital-based AYA cancer programs with dedicated staff providing developmentally appropriate, customized care to AYA patients. We have also seen the establishment of community advocacy and philanthropic organizations to support improved access to AYA cancer care and an increase in research examining both the biopsychosocial underpinnings of AYA cancer and the experiences of AYA patients with cancer across the treatment trajectory.
Clinical trial participation, which offers patients access to newer and potentially more effective treatments, is lower among AYAs than among both older and younger patients; some estimates suggest that just 2% to 5% of eligible AYAs participate in clinical trials.16-19
While early in development, efforts to formalize training in AYA oncology are underway. Work is still needed to ensure that AYAs have equitable access to tailored care and research opportunities; however, efforts thus far have changed the landscape of AYA cancer. Some successes include:
- Advanced treatment options to promote AYA-targeted therapies and the use of precision medicine to reduce treatment-related side effects
- Expanded recognition of the importance of survivorship care and the transition to post-treatment life
- Increased clinical trial access with AYA-inclusive age ranges
- Enhanced psychosocial support mechanisms through the integration of mental health services, peer support programs, and online communities into cancer care.
The UNC Lineberger Adolescent and Young Adult Cancer Program
Since its founding in 2015, the University of North Carolina at Chapel Hill (UNC) Lineberger Adolescent and Young Adult Cancer Program has grown from a team of 1 to a multidisciplinary group of 11 individuals who have the common goal of improving access, experiences, and outcomes for AYAs with cancer at the North Carolina Basnight Cancer Hospital, UNC Children’s Hospital, and beyond. The reach of our program has grown consistently over the past decade thanks to increasingly operationalized partnerships with philanthropic partners (eg, Teen Cancer America, Be Loud! Sophie Foundation), other care teams, buy-in from leadership, community support, and recognition of the value of this program within UNC’s hospital system more broadly. Below, contextualized in an overview of AYAs’ unique needs, we summarize the latest research and practices, clinical standards, and practical tips for working with this patient population. We also present ongoing efforts of our program, highlighting some ways we strive to better understand and support our patients. As a large, academic medical center that serves all 100 counties of North Carolina, we recognize that the context of our work may differ vastly from that of many community programs. We hope that the information presented here provides relevant evidence and actionable tips for providers caring for AYAs with cancer in any setting.
AYA’s Unique Characteristics: Unified by Circumstantial Age
Our team members are often asked questions like, “Why is the AYA population defined by the ages of 15 to 39 years?” or “What does a 15-year-old high school student who lives with her parents have in common with a 35-year-old mother of 2 who works full-time?” There are significant variations in cancer experience across this age range, and many experts in the field are beginning to consider 3 distinct AYA subgroups—adolescents (age, ≈ 15-19 years), emerging adults (age, ≈ 20-29 years), and young adults (age, ≈ 30-39 years)—all made up of young individuals diagnosed with cancer and struggling with the impact that their disease and its treatment has on core developmental milestones. In a seminal article considering how best to define the AYA population, Kristin McMaster, MSW, aptly used the term circumstantial age. McMaster argued that understanding the unique psychosocial needs of an individual with cancer is more informative than is consideration of chronological age.5 AYAs are bound by many unique life transitions: completing education, establishing a career, building social systems and personal relationships, achieving financial and housing independence, and building a family. Cancer treatment can derail any and all of these milestones, creating a set of needs distinct from that of older or younger individuals.
For instance, as most AYAs have not achieved career and financial independence, a cancer diagnosis can lead to lifelong disruption of professional and financial well-being. Financial toxicity, which the NCI defines as the “problems a patient has related to the cost of medical care,” impacts AYA patients at higher rates than it does older patients.6 Among AYAs, this financial hardship has been associated with skipping or delaying necessary medical, mental health, and survivorship care as well as having negative impacts on long-term financial health including reduction in credit scores, higher risk for bankruptcy, and increased debt burden.7 Like the disruption to other developmental milestones caused by a cancer diagnosis during formative years, AYAs with cancer may face delays, interruptions, or alterations to their educational pursuits, graduation timelines, and workforce entry/advancement, all of which inhibit the attainment of financial independence typically associated with young adulthood.
In addition to unique psychosocial impacts of a cancer diagnosis, there are distinct biological factors underpinning AYA cancers that may contribute to poorer outcomes.8,9 For instance, there is growing awareness of the increasing incidence of cancers such as those of the colorectal or breast earlier in life. As compared to cancers in older adults, young adult–onset cancers are disproportionately associated with high-risk biological or genetic features such as mucinous histology, signet ring presence, or mismatch gene repair mutations in colorectal cancer and triple-negative hormone receptor status in breast cancer, all of which are associated with poorer survival outcomes. Compared with younger children with acute lymphoblastic leukemia (ALL), AYAs are more likely to have a Philadelphia chromosome–positive (Ph+) or Ph-like variant (gene expression similar to that of Ph+ without the BCR-ABL translocation), both of which are associated with higher mortality rates. Efforts to target these molecular changes (eg, inclusion of BCR-ABL tyrosine kinases for treatment of AYAs with Ph+ disease) have begun to improve outcomes. Additional work is needed to more comprehensively define the unique histological and genetic landscape of AYA cancers, to map these to the most appropriate therapies that target these biologically distinct diseases, and to better understand the interactions between tumor biology and outcomes among AYAs.
Adverse health outcomes are common in the growing population of AYA cancer survivors, leading to decades of impaired QOL, disability, morbidity, and early mortality. Although AYAs represent a small proportion of the overall cancer survivor population, they disproportionately experience poor outcomes including higher rates of cancer-related distress, mental health impairment, and severe and life-threatening conditions compared to other cancer survivor populations.10-12 A 2013 Institute of Medicine report, Identifying and Addressing the Needs of Adolescents and Young Adults with Cancer, recognized the improvement of survivorship care as a priority area; further, it specifically recommended that AYA survivor cohorts be established to facilitate the development of guidelines to follow this at-risk population over the long term.4 This is an area of active research to examine the health and well-being of survivors of AYA cancers that is distinct from efforts for childhood or older adult cancer survivors.

Considerations for Providers: Select Issues in AYA Care
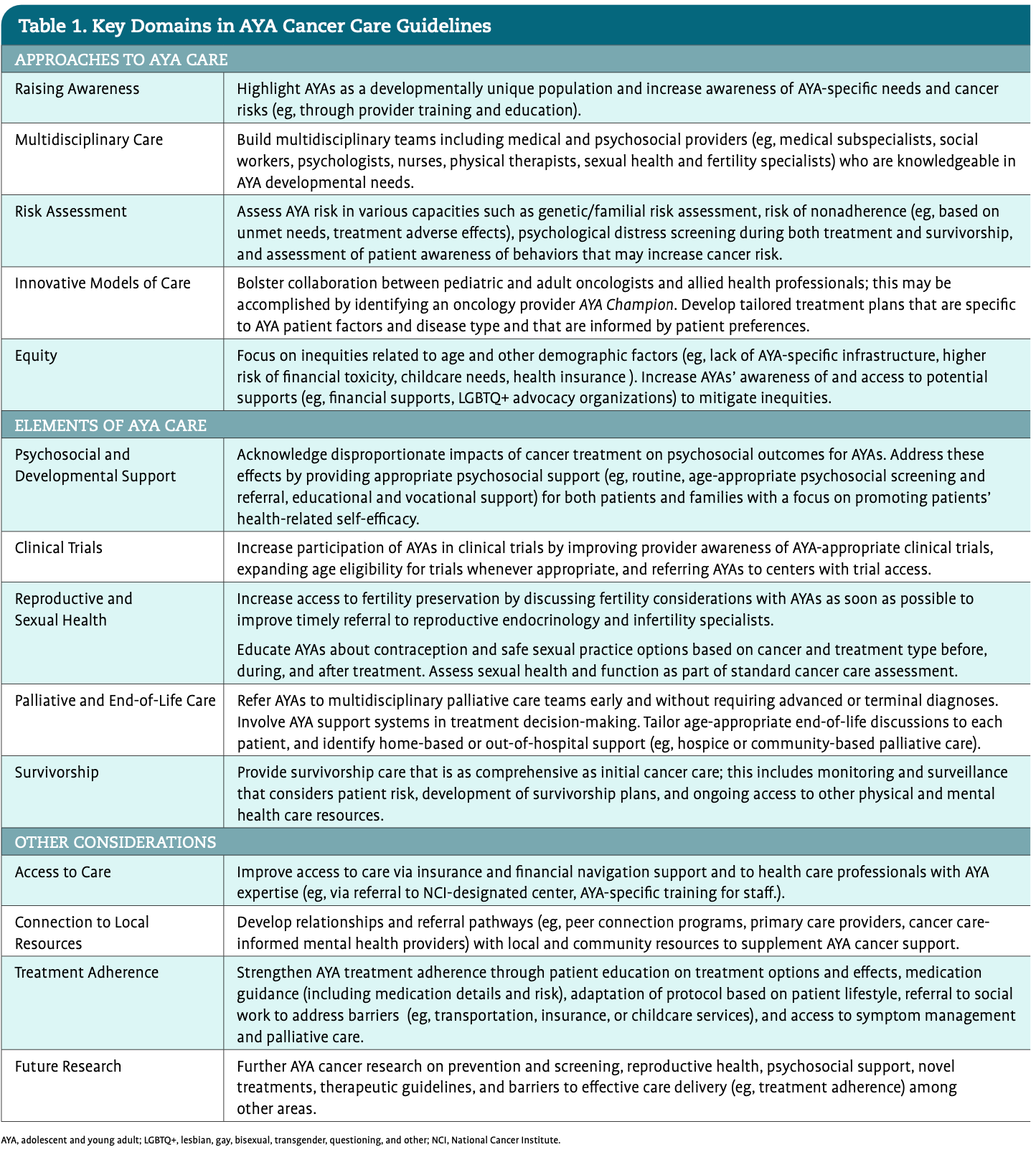
Understanding the unique characteristics of the AYA population is an essential first step in providing them with excellent cancer care. Based on these unique biopsychosocial needs, we highlight select areas for consideration below, building on the experiences of our AYA cancer team over the last 9 years and focusing on actionable areas for clinicians. While many of these topics are relevant across all age groups, we find that they are specifically pertinent to enhancing cancer outcomes among AYAs. Beyond these select considerations, Table 1 provides providers with an overview of cross-cutting care considerations in AYA cancer care.

Fertility
Addressing fertility for young patients is paramount. While there is not a precise overlap between the standard AYA age range and reproductive age, there is expert and guideline consensus that anyone of childbearing age should be educated about the potential effects of cancer and cancer treatment on future fertility.13,14 The influence of cancer treatment on future fertility is difficult to study and precisely quantify, but chemotherapy—particularly regimens containing alkylators—increases the risk of ovarian dysfunction and diminishes sperm production. Pelvic radiation and certain gynecologic and urologic surgeries can also affect fertility potential. While some AYAs recover reproductive organ function, other patients may permanently lose the ability to have biological children after cancer treatment. This outcome is a cause for significant emotional distress for many AYAs, and it is frequently mentioned as a top concern for young people facing cancer. The essential takeaways for providers are 2-fold. First, there are a range of options available for fertility preservation. Second, a conversation about those options can be tremendously reassuring in the long term regardless of the path the patient chooses to take.
A comprehensive review of fertility preservation options is beyond the scope of this article. However, practical guidelines have been published that can be referenced when these cases arise. In 2023, Hoffman et al published an excellent “Viewpoint” in JAMA Oncology that offered strategies for fertility preservation in an easily digestible format.15 Briefly, these experts recommended early introduction of fertility discussions and prompt referral to fertility specialists for interested patients. Importantly, many of these treatments can be completed quickly—some within 24 hours (eg, sperm banking, leuprolide ovarian suppression) and others within a few days to 2 weeks. Some options are typically excluded from insurance coverage and carry substantial financial barriers, but many cancer programs and nonprofit organizations offer resources to help defray out-ofpocket costs. Clear communication and care coordination are essential, and it is worth revisiting fertility considerations and family planning options at transitional time points before, during, and after cancer treatment, since questions, concerns, or the degree of psychosocial distress may evolve as the patient progresses through treatment and survivorship. Although a patient may not use fertility preservation therapies at diagnosis, this does not mean that many treatments (eg, sperm banking, egg cryopreservation) would not remain options later in survivorship.
Spaces that promote interconnectedness and that give AYAs the opportunity to engage or be present with other AYA cancer patients are beneficial whenever possible.32
Clinical Trial Participation
Clinical trial participation, which offers patients access to newer and potentially more effective treatments, is lower among AYAs than among both older and younger patients; some estimates suggest that just 2% to 5% of eligible AYAs participate in clinical trials.16-19 Limited clinical trial participation likely is a significant driver of the lack of overall improvement in outcomes for AYAs as compared with members of other age groups. Clinical trial participation among AYAs is hampered by eligibility criteria that are based on numerical age rather than biological or metabolic mechanisms and by limited physician awareness of AYA trials owing, in part, to a lack of a comprehensive AYA clinical trials registry. Adolescent patients also face barriers relating to slower drug development times and the additional clinician effort required to enroll minors onto clinical trials.20,21 Efforts are ongoing to improve AYA clinical trial participation; these include increasing access to trials through community-based cooperative groups such as the NCI Oncology Community Research Program (NCORP), developing intergroup trials focusing on AYA cancers that leverage pediatric and adult oncology infrastructure, and expanding health insurance coverage as through the Affordable Care Act.16 Providers can help increase participation of AYAs in clinical trials by expanding their own awareness of AYA-appropriate clinical trials, being an institutional advocate for activation of clinical trials for AYAs, establishing relationships with colleagues at cancer centers where AYA trials may be more available, and referring patients to centers with trial access when possible.
Treatment Planning and Adjustment
Consideration of long-term side effects and toxicities of therapies is particularly important for young patients. For the oncology provider, side effects and toxicities of therapy carry several important implications. First, these potential concerns merit in-depth discussion with AYAs. However, patients may not process the potential long-term complications of therapy at the outset of treatment for a lifethreatening malignancy. Returning to these discussions after treatment and encouraging enhanced surveillance for late effects in the survivorship phase is key to managing potential comorbidities should they arise. Second, spending extra time in the treatment planning phase to weigh the absolute risk of recurrence or death from cancer with the risks of long-term treatment-related harms is warranted. Often, these discussions are best led by providers who regularly provide care for and are well versed in the nuances of the specific AYA cancer in question and are ideally supported by high quality evidence. De-escalation of therapies can be considered in some cases. For instance, decreasing the use of radiation to treat Hodgkin lymphoma has led to a reduction in long-term harm while maintaining excellent survival outcomes. We encourage oncologists who do not routinely care for AYAs to contact AYA-experienced colleagues or to participate in AYA tumor boards for advice when developing a treatment plan to ensure the provision of the best possible care.
Survivorship
Comprehensive and timely survivorship care is critical for AYAs, since late effects may develop for decades following treatment. Despite this, many AYAs may not receive survivorship care focused on enhancing QOL, health span, and lifespan. Comprehensive survivorship care resources are limited at many cancer programs, and this population often faces financial and informational barriers in accessing this care. An essential first step is ensuring AYA survivors are connected to a primary care provider (PCP), which may involve social work or financial services to facilitate access. Clinicians can also provide counseling about the importance of ongoing survivorship care during active treatment, enhance communication between patients and their PCP by creating a survivorship care plan, and connect AYAs to national resources for AYA cancer survivors (Table 2). Additionally, survivorship care guidelines, such as those developed by the NCCN and the Children’s Oncology Group, offer guidance to providers in navigating comprehensive care provision (Table 2)


Health Insurance
Insurance is a frustrating and common challenge when caring for young patients with cancer. Of course, this problem is not limited to AYAs; however, when looking at the US as a whole, young adults are the most frequently uninsured patient population.22 This factor can lead to delays in diagnosis and limited access to appropriate specialists or supportive care services, and it is ultimately associated with worse cancer survival.23 In addition, a lack of experience in navigating health care services means that AYAs often do not know how to advocate for themselves or manage insurance applications or claims appeals, and they may get stuck with inappropriately high-cost care without the right supports to navigate their options. Thus, it is worth anticipating these challenges, asking about financial barriers and insurance access, and engaging AYAs with financial services and social work early in their disease course to try to prevent these issues. On a policy level, we encourage clinicians and oncology advocacy groups to continue to push for expanded insurance access and coverage for patients generally but especially for young people who are particularly vulnerable to gaps in insurance.
Comprehensive Considerations
A number of comprehensive guidelines on AYA cancer care have been published over the past 15 years spanning medical care, psychosocial care, advocacy and research efforts, and beyond.19-21,24-28 Although these guidelines vary in content and depth, there are overlapping domains that warrant the attention of any providers working with AYA patients. These key areas of overlap are summarized in Table 1. Additionally, a scoping review of these guidelines is currently underway; our team anticipates that it will be published over the next year.
Practical Considerations for Working with AYAs
AYA Care Delivery
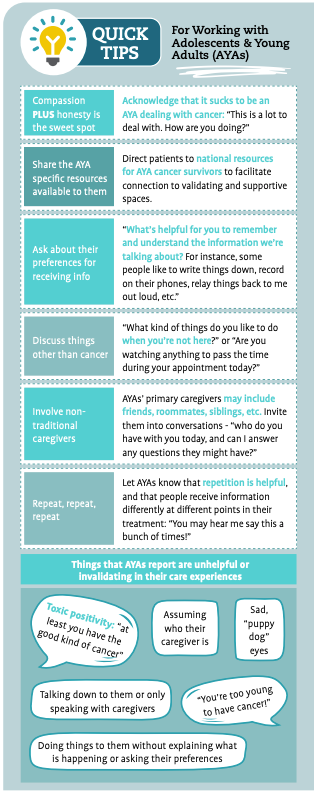
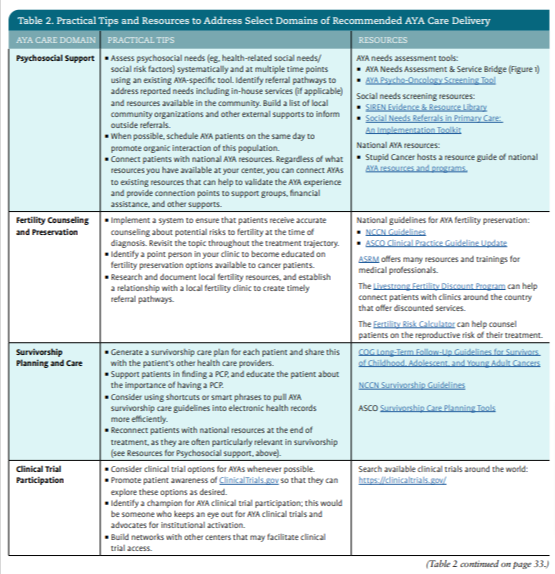
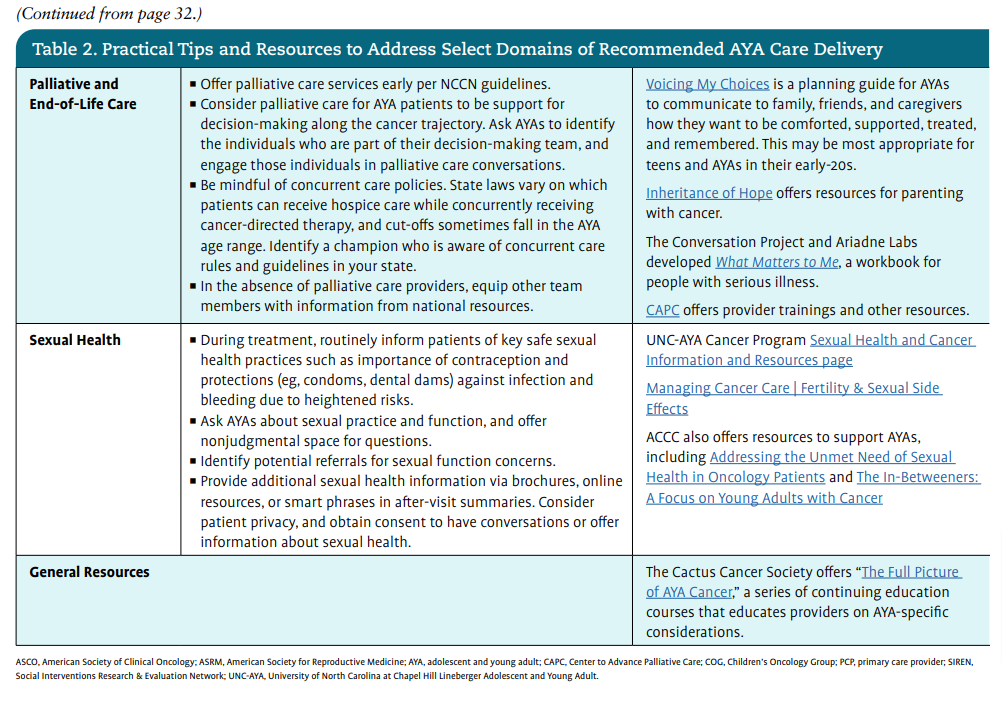
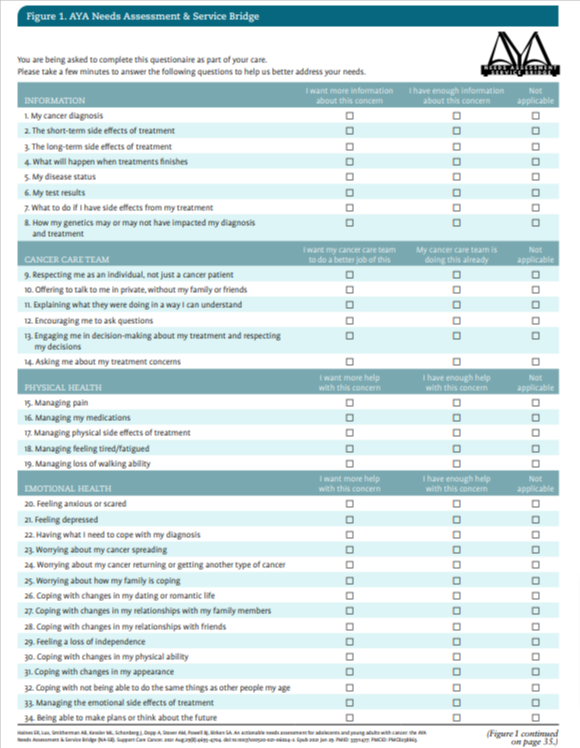
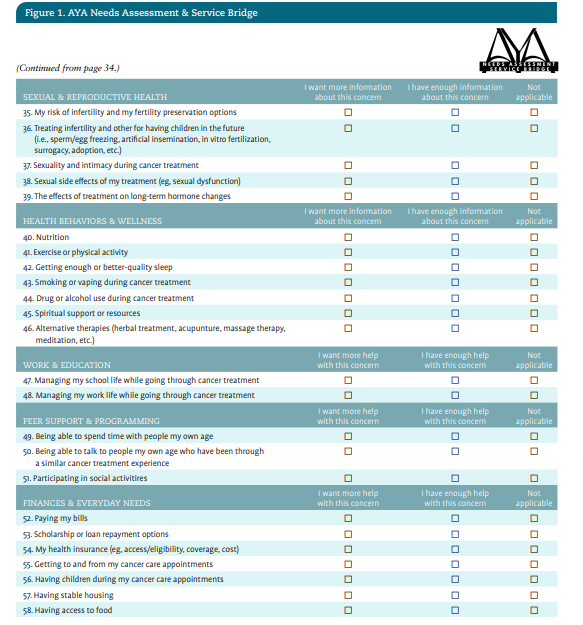
We recognize that while guidelines for optimal AYA cancer care are increasingly available, adherence to these guidelines may be suboptimal in part because of a lack of concrete steps and resources for meeting these guidelines. In Table 2, we offer practical tips for addressing select domains of AYA care including both clinical and program development tips. On page 29 of this article, you will find a handout highlighting additional tips for direct patient interaction.


AYA Program Implementation
Across the country, we are seeing dedicated AYA cancer programs emerge. Importantly, you do not need to have a formalized AYA program or AYA-specific staff to integrate some of the tips above into your practice. However, there are resources available to guide these efforts if your center is interested in building out specialized care for AYAs. Hospitals and health systems can seek support from Teen Cancer America, a nonprofit foundation that provides seed funding and consultation services to hospitals around the country seeking to develop AYA cancer programs.29 Additional resources are available that describe barriers to implementation of AYA programs, strategies to address these obstacles,30 and practical lessons learned in program development.31
UNC Lineberger’s Adolescent and Young Adult Cancer Program: Ongoing Efforts
Our program has grown over the past decade, and we have worked to find ways to better understand and support AYA patients and survivors. Below, we offer a few examples of program and research initiatives that our team has undertaken with the invaluable collaboration of partners and patients.
Survivorship Clinic Development
In recent years, we launched a transition and survivorship clinic to meet the diverse needs of AYA cancer survivors as they complete active therapy. This clinic was created in partnership with AYA survivors on our Young Adult Advisory Board to recognize the complex, multifaceted nature of AYA survivorship. Based on feedback from these patient advocate partners concerning potential medical trauma associated with the cancer center, our clinic was strategically located outside the cancer center to ensure that patients do not need to return to their treatment site. Survivorship care visits are jointly conducted with our AYA clinical social worker and an AYA medical provider (MD or NP) to ensure comprehensive needs assessment. Survivors are offered health education and referrals for services such as cancer rehabilitation, mental health care, or additional health screening and provided with a detailed survivorship care plan and AYA support resources.
AYA-Specific Spaces
Guidance on AYA care emphasizes a need for environments that are designed specifically with this population in mind.20,28 Spaces that promote interconnectedness and that give AYAs the opportunity to engage or be present with other AYA cancer patients are beneficial whenever possible.32 Over the years, patients have told us how isolated they feel as they sit in infusion spaces surrounded by significantly older adults. In partnership with the Be Loud! Sophie Foundation, First Citizens Bank, and Teen Cancer America, our Be Loud! Center for Young Adult Care opened in November 2023. This infusion space is designed specifically for young adult patients. As with our survivorship clinic, the conceptualization and creation of this space closely involved guidance from our Young Adult Advisory Board. The efforts of the board, the AYA team, and our partners resulted in the infusion center pictured on page 28. It incorporates design elements of nature, 2 (rather than 1) chairs for support people, moveable screens, and a café seating area where patients and caregivers can connect. Our team is excited about this space and the opportunities it offers for peer support, centralized programming, AYA-trained staff, and research. However, we also strongly believe that having a dedicated space is not a prerequisite to improving care for this population. Similar goals can be achieved by using the tips shared above such as scheduling AYAs on the same clinic days to offer opportunities for organic connection.
Research Agenda
While we believe access to a space such as this will improve the overall patient treatment experience, we are testing this hypothesis in a current study. Our infusion space study aims to understand the impacts of the new infusion space on patient experience. We employed surveys and ethnographic interviews administered before treatment to gather patients’ perspectives on their experiences in general adult infusion spaces prior to their use of the AYA-specific space. As the space becomes fully operational, we will conduct follow-up surveys and ethnographic interviews to allow for a comparison of patient experiences in these different spaces. Our hope is that this research will inform both future adaptations to the Be Loud! Center for Young Adult Care and the work of other health care settings who plan to implement similar changes to their built environments.
Within our institution, the monthly UNC AYA Research Working Group brings together research and clinical personnel across the UNC campus and beyond to share and receive feedback on works in progress and collaborate on prospective projects.
In addition to efforts focused specifically on our infusion space, our research agenda includes a formalized understanding of our program reach and impact more broadly. An ongoing UNC AYA Program Pilot Study uses electronic health record data linked with those from the North Carolina Cancer Registry to better characterize AYA patients in our cancer program, understand which patients engage with our team, describe the services that we are providing to AYAs, and evaluate the impact of the AYA Cancer Program on AYA-specific cancer outcomes. Ideally, the findings from this study will support other health care settings in developing their own AYA program by demonstrating the effectiveness of investment in this model of care.
As discussed above, the unique developmental position of AYAs means that the survival horizon of this population is lengthy. Most AYAs with cancer will be cured of their disease and survive well into adulthood. Thus, mitigating long-term effects of cancer care for this population is crucial. The UNC Childhood, Adolescent and Young Adult Cancer Cohort (UNC-CAYACC [NCT05096923]) is a first-of-its-kind study that tracks patients from diagnosis through survivorship with a focus on describing the pro-aging effects of cancer and its treatments. The study aims to associate measures of aging and QOL with cancer, treatment, and psychosocial factors. We are hopeful that these and other research efforts will directly impact young people’s cancer outcomes and QOL.
Transdisciplinary Collaboration
Much of our program’s impact is driven by AYA-focused collaborations across teams and institutions. An early goal of the program was to engage in transdisciplinary education across the state; this goal was reached by the North Carolina AYA Oncology Symposium. This annual full-day symposium is a collaborative effort that also involves the Mountain Area Health Education Center and AYA programs at UNC Lineberger Cancer Center, Duke Cancer Institute, and Atrium Health Wake Forest Baptist. Increasingly, AYA champions in research and clinical care at other North Carolina cancer programs have contributed as presenters and symposium planners. Symposium agendas thus far have focused on sharing best practices in a variety of clinical care areas across the treatment trajectory and on exploring research and advocacy efforts in AYA oncology locally and nationwide. Within our institution, the monthly UNC AYA Research Working Group brings together research and clinical personnel across the UNC campus and beyond to share and receive feedback on works in progress and collaborate on prospective projects.
Our program has also formed various clinical initiatives. These include AYA disease group summits that bring together pediatric and adult providers to establish institutional best practices and enhance clinical trial enrollment. In addition, a clinical collaborative introduces palliative care and psychosocial services to high-need YA sarcoma patients at diagnosis. Our team also participates in a monthly AYA Molecular and Medical Tumor Board led by partners at Bon Secours Mercy Hospital in Greenville, South Carolina, which brings together AYA experts from community and academic centers across the southeast to promote high-quality, AYA-focused cancer care. These initiatives, among others, open avenues for engagement in AYA efforts that extend beyond the bounds of a formal AYA program.
Final Thoughts
We have been fortunate at UNC to have the institutional and community support to build a robust AYA oncology program. We recognize that the majority of AYAs receive cancer care in settings that may currently lack the buy-in or resources for a dedicated AYA team. The models of care that have been effective here may not be replicable, and they may not best serve the needs of different institutions and patient populations. However, we have learned from our partners and patients that any cancer program can improve care for this population through incremental adjustments and a commitment to exploring the unique needs of AYAs. The information we have provided here is a brief survey of a complex and ever-growing body of evidence that points to the importance of unique approaches to care for this population. We hope that the summaries, resources, and practice recommendations shared here can be helpful to other cancer centers as they refine their own unique approaches to the provision of high-quality, tailored AYA cancer care.
Hannah C. Winslow, MSW, MPH, is the AYA project manager at UNC’s AYA Cancer Program in Chapel Hill, North Carolina. Catherine Swift, MSW, LCSW, is the AYA clinical social worker at UNC’s AYA Cancer Program in Chapel Hill, North Carolina. Jacob N. Stein, MD, MPH is the AYA oncology liaison at UNC’s AYA Cancer Program in Chapel Hill, North Carolina. Emily R. Haines, PhD, is the research director at UNC’s AYA Cancer Program in Chapel Hill, North Carolina and an assistant professor at Wake Forest University School of Medicine in Wake Forest, North Carolina. Bridgette Thom, PhD, is an assistant professor at the UNC School of Social Work in Chapel Hill, North Carolina. Lauren Lux, MSW, LCSW, is the former program director at UNC’s AYA Cancer Program in Chapel Hill, North Carolina. Alison Manikowski, PsyD, is the pediatric psychologist at UNC’s AYA Cancer Program in Chapel Hill, North Carolina. Aspen Yordy, MS, CCLS, is the AYA research coordinator at UNC’s AYA Cancer Program in Chapel Hill, North Carolina. Jordan Lodato Hunt, LCSW, is the fertility preservation program director at UNC’s AYA Cancer Program in Chapel Hill, North Carolina. Melissa Matson, MSN, RN AGPNP-BC, AOCNP, is the AYA nurse practitioner at UNC’s AYA Cancer Program in Chapel Hill, North Carolina. Andrew B. Smitherman, MD, MSc, is the AYA medical director at UNC’s AYA Cancer Program in Chapel Hill, North Carolina.
References
1. Page LL, Devasia TP, Mariotto A, Gallicchio L, Mollica MA, Tonorezos E. Prevalence of cancer survivors diagnosed during adolescence and young adulthood in the United States. J Natl Cancer Inst. 2024 Oct 9:djae250. doi:10.1093/jnci/djae25
2. National Cancer Institute. Cancer stat facts: cancer among adolescents and young adults (AYAs) (ages 15–39). Surveillance, Epidemiology, and End Results Program. 2020. Accessed December 16, 2024. https://seer.cancer.gov/ statfacts/html/aya.html
3. Armenian SH, Chao C. Burden of morbidity and mortality in adolescent and young adult cancer survivors. J Clin Oncol. 2024;42(6):735-742. doi:10.1200/JCO.23.01751
4. Nass SJ, Beaupin LK, Demark-Wahnefried W, et al. Identifying and addressing the needs of adolescents and young adults with cancer: summary of an Institute of Medicine workshop. Oncologist. 2015;20(2):186-195. doi:10.1634/theoncologist.2014-0265
5. McMaster K. What should the age range be for AYA oncology? J Adolesc Young Adult Oncol. 2011;1(1):3-10. doi:10.1089/jayao.2011.1505
6. Financial toxicity (financial distress) and cancer treatment (PDQ)–patient version. General information about financial toxicity (financial distress) and cancer treatment. National Cancer Institute. Accessed December 16, 2024. https://www.cancer.gov/about-cancer/managing-care/track-care-costs/ financial-toxicity-pdq
7. Thom B, Benedict C. The impact of financial toxicity on psychological well-being, coping self-efficacy, and cost-coping behaviors in young adults with cancer. J Adolesc Young Adult Oncol. 2019;8(3):236-242. doi:10.1089/ jayao.2018.0143
8. Close AG, Dreyzin A, Miller KD, Seynnaeve BKN, Rapkin LB. Adolescent and young adult oncology-past, present, and future. CA Cancer J Clin. 2019;69(6):485-496. doi:10.3322/caac.21585
9. Tricoli JV, Bleyer A. Adolescent and young adult cancer biology. Cancer J. 2018;24(6):267-274. doi:10.1097/PPO.0000000000000343
10. Smith AW, Keegan T, Hamilton A, et al; AYA HOPE Study Collaborative Group. Understanding care and outcomes in adolescents and young adult with cancer: a review of the AYA HOPE study. Pediatr Blood Cancer. 2019;66(1):e27486. doi:10.1002/pbc.27486
11. Zebrack B. Information and service needs for young adult cancer survivors. Support Care Cancer. 2009;17(4):349-357. doi:10.1007/ s00520-008-0469-2
12. Chao C, Bhatia S, Xu L, et al. Chronic comorbidities among survivors of adolescent and young adult cancer. J Clin Oncol. 2020;38(27):3161-3174. doi:10.1200/JCO.20.00722
13. Oktay K, Harvey BE, Partridge AH, et al. Fertility preservation in patients with cancer: ASCO clinical practice guideline update. J Clin Oncol. 2018;36(19):1994-2001. doi:10.1200/JCO.2018.78.1914
14. Bhatia S, Pappo AS, Acquazzino M, et al. Adolescent and young adult (AYA) oncology, version 2.2024, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2023;21(8):851-880. doi:10.6004/ jnccn.2023.0040
15. Hoffman AS, Rauh-Hain JA, Woodard TL. Preserving fertility in women with cancer: practice strategies. JAMA Oncol. 2023;9(1):21-22. doi:10.1001/ jamaoncol.2022.4930
16. Keegan THM, Parsons HM. Adolescent angst: enrollment on clinical trials. Hematology Am Soc Hematol Educ Program. 2018;2018(1):154-160. doi:10.1182/asheducation-2018.1.154
17. Bleyer A. Older adolescents with cancer in North America deficits in outcome and research. Pediatr Clin North Am. 2002;49(5):1027-1042. doi:10.1016/s0031-3955(02)00035-4
18. Tai E, Buchanan N, Westervelt L, Elimam D, Lawvere S. Treatment setting, clinical trial enrollment, and subsequent outcomes among adolescents with cancer: a literature review. Pediatrics. 2014;133(suppl 3):S91-S97. doi:10.1542/peds.2014-0122C
19. Patterson P, Allison KR, Bibby H, et al. The Australian Youth Cancer Service: developing and monitoring the activity of nationally coordinated adolescent and young adult cancer care. Cancers (Basel). 2021;13(11):2675. doi:10.3390/cancers13112675
20. Ferrari A, Stark D, Peccatori FA, et al. Adolescents and young adults (AYA) with cancer: a position paper from the AYA Working Group of the European Society for Medical Oncology (ESMO) and the European Society for Paediatric Oncology (SIOPE). ESMO Open. 2021;6(2):100096. doi:10.1016/j.esmoop.2021.100096
21. Smith AW, Seibel NL, Lewis DR, et al. Next steps for adolescent and young adult oncology workshop: an update on progress and recommendations for the future. Cancer. 2016;122(7):988-999. doi:10.1002/cncr.29870
22. Vaca Lopez PL, Warner EL, Waters AR, et al. Adaptation and development of a health insurance education program for adolescent and young adult cancer patients. J Adolesc Young Adult Oncol. 2023;12(5):692-700. doi:10.1089/jayao.2022.0103
23. Rosenberg AR, Kroon L, Chen L, Li CI, Jones B. Insurance status and risk of cancer mortality among adolescents and young adults. Cancer. 2015;121(8):1279-1286. doi:10.1002/cncr.29187
24. Coccia PF, Pappo AS, Beaupin L, et al. Adolescent and young adult oncology, version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2018;16(1):66-97. doi:10.6004/jnccn.2018.0001
25. Smith S, Mooney S, Cable M, Taylor RM. The Blueprint of Care for Teenagers and Young Adults with Cancer. 2nd ed. Smith S, Mooney S, Cable M, Taylor RM, eds. Teen Cancer Trust; 2016. Queen’s University Belfast. Accessed December 17, 2024. https://pure.qub.ac.uk/files/128955595/TCT_ Blueprint_31_10_2016.pdf
26. Fernandez C, Fraser GAM, Freeman C, et al. Principles and recommendations for the provision of healthcare in Canada to adolescent and young adult-aged cancer patients and survivors. J Adolesc Young Adult Oncol. 2011;1(1):53-59. doi:10.1089/jayao.2010.0008
27. Hovsepyan S, Hoveyan J, Sargsyan L, et al. The unique challenges of AYA cancer care in resource-limited settings. Front Adolesc Med. 2023;1. doi:10.3389/fradm.2023.1279778
28. Rajani S, Young AJ, McGoldrick DA, Pearce DL, Sharaf SM. The international charter of rights for young people with cancer. J Adolesc Young Adult Oncol. 2011;1(1):49-52. doi:10.1089/jayao.2010.0007
29. Haines ER, Gan H, Kupelian A, et al. The development and implementation of adolescent and young adult oncology programs: Teen Cancer America’s strategy. J Adolesc Young Adult Oncol. 2024;13(2):347-351. doi:10.1089/jayao.2023.0110
30. Haines E, Asad S, Lux L, et al. Guidance to support the implementation of specialized adolescent and young adult cancer care: a qualitative analysis of cancer programs. JCO Oncol Pract. 2022;18(9):e1513-e1521. doi:10.1200/OP.22.00063
31. Haines ER, Lux L, Stein J, et al. Developing a comprehensive adolescent and young adult cancer program: lessons learned from 7 years of growth and progress. J Adolesc Young Adult Oncol. 2023;12(6):868-878. doi:10.1089/ jayao.2023.0015
32. Zebrack B, Mathews-Bradshaw B, Siegel S, LIVESTRONG Young Adult Alliance. Quality cancer care for adolescents and young adults: a position statement. J Clin Oncol. 2010;28(32):4862-4867. doi:10.1200/ JCO.2010.30.5417


")

")



")





")